C. Blastomere size
"STAGE SPECIFIC" VERSUS "NON-STAGE SPECIFIC"
It has been shown that a high degree of regularity in the blastomere size in embryos on Day 2 is related to increased pregnancy outcome following assisted reproduction treatments (Giorgetti et al., 1995; Ziebe et al., 1997; Hardarson et al., 2001; Holte et al., 2007). Uneven cleavage, i.e. a cell cleaving into two unequal sized cells, may result in an uneven distribution of cytoplasmic molecules, e.g. proteins and mRNAs, and has been shown to be correlated with a higher incidence of multinucleation and aneuploidy (Hardarson et al., 2001; Magli et al., 2001).
The relative blastomere size in the embryo is dependent on both the cleavage stage and the regularity of each cleavage division (Diagrams 1 and 2). The blastomeres of 2-, 4- and 8-cell embryos should be equal (stage-specific embryos, Figs 243–245) rather than unequal in size (non-stage-specific embryos, Figs 246–252). In contrast, blastomeres of embryos with cell numbers other than 2, 4 and 8 should have different sizes as there is an asynchrony in the division of one or more blastomeres (Figs 253–256). A 3-cell embryo should preferably have one large and two small blastomeres (Fig. 253); a 5-cell embryo, three large and two smaller blastomeres (Fig. 254); a 6-cell embryo, two large and four smaller blastomeres (Fig. 255) and a 7-cell embryo, one large and six smaller blastomeres (Fig. 256). These embryos are thereby also considered to be stage specific. However, a 4-cell embryo with one or two blastomers much larger than the others (Figs 248–251), a 3-cell embryo with all blastomeres even in size (Fig. 257), a 5-cell embryo with two large and three smaller blastomeres (Figs 258 and 259) or one small and four larger blastomeres (Fig. 260), a 6-cell embryo with all blastomeres even in size (Fig. 261) or extremely different in size (Fig. 262) and a 7-cell embryo with three large and four smaller blastomeres (Fig. 263) would not be considered to have normal blastomere sizes in relation to cell numbers and are therefore not considered to be stage specific (for further clarification see Diagrams 1 and 2).
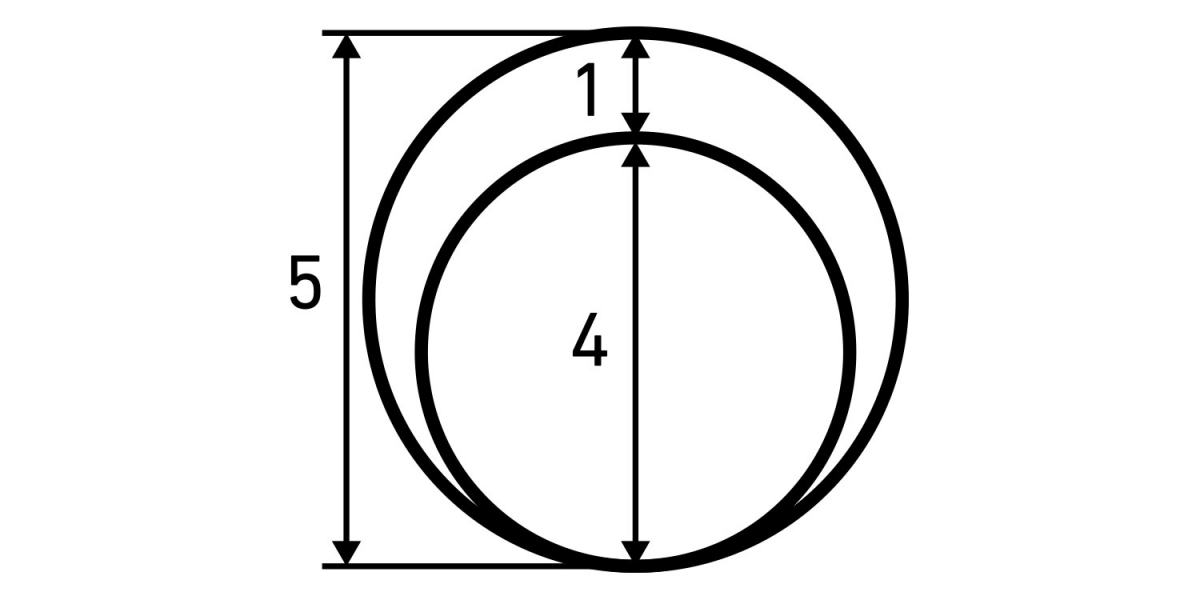
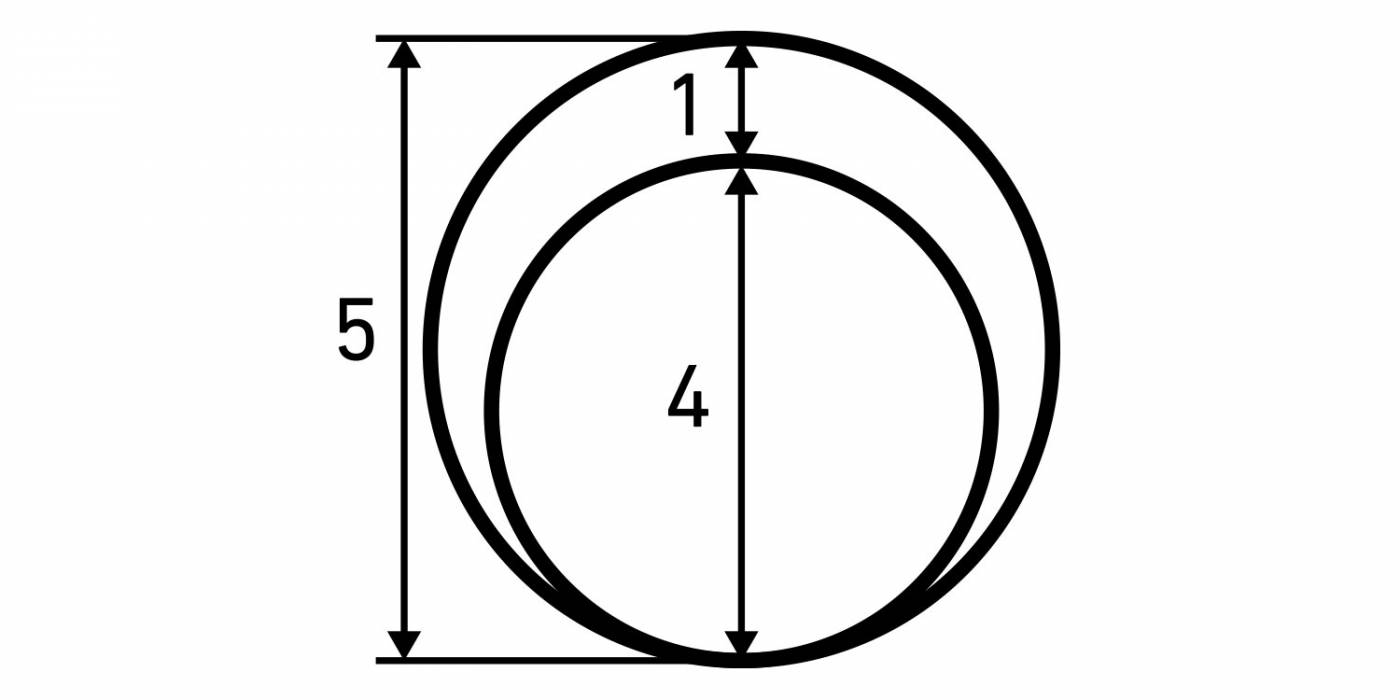
Diagram 1
A diagram illustrating the expected cell size of a cleavage stage embryo: a human 2-cell embryo should contain two equal blastomeres of the size of the 2-cell stage and are thereby stage specific. Unequal blastomeres at the 2-cell stage (>25% difference in the diameter size of the smallest cell, i.e. less than a 1:4 proportion) are not 2-cell stage specific. The same rule can be applied to 4- and 8-cell embryos. The numbers show proportions of diameter size.
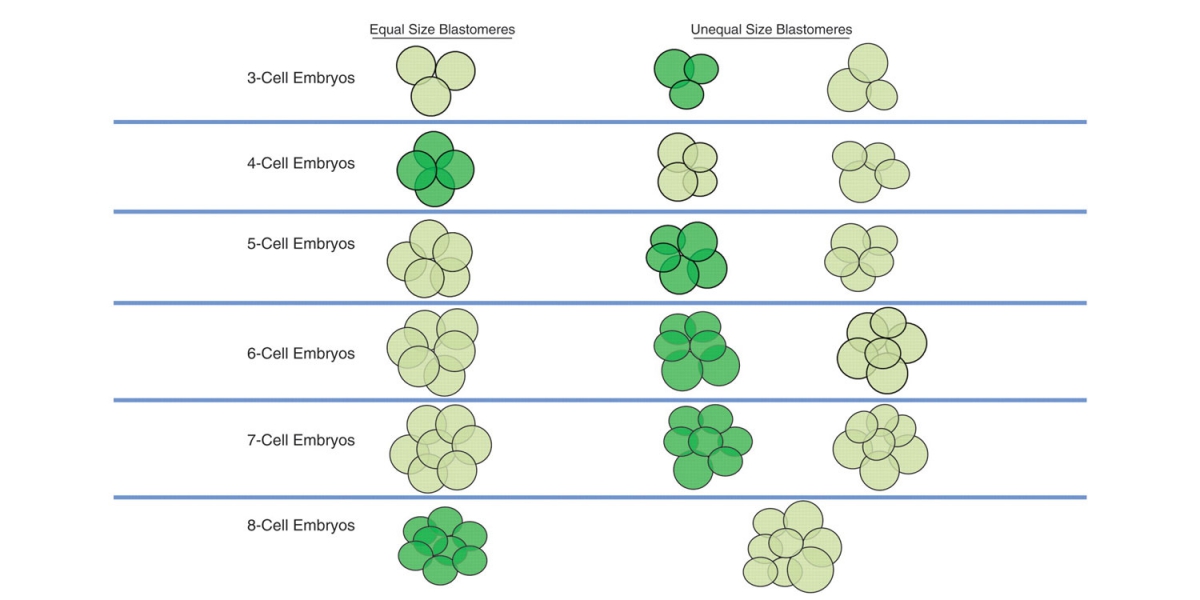
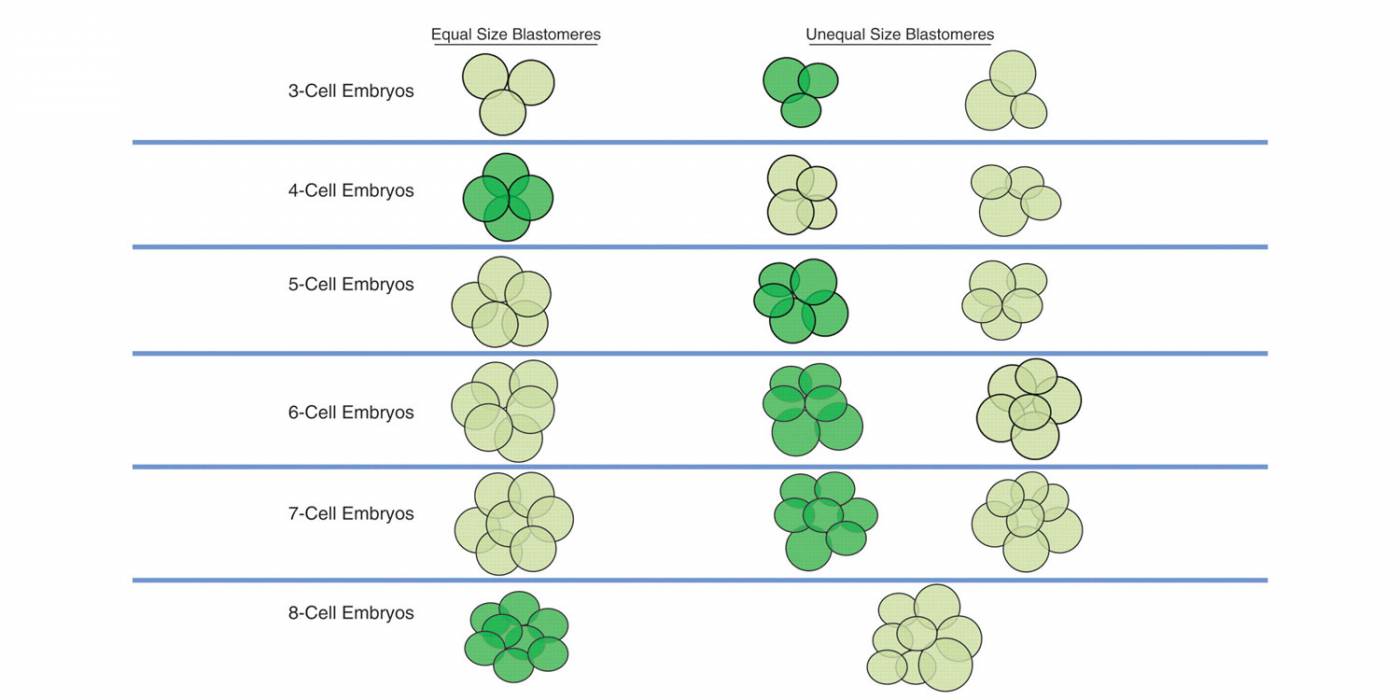
Diagram 2
A diagram illustrating the concept of stage-specific versus non-stage-specific cleavage patterns. The dark green color indicates stage-specific cleavage stage embryos, whereas the light green color indicates non-stage-specific cleavage stage embryos.


Figure 243
A 2-cell embryo with evenly sized blastomeres and no fragmentation on Day 2. The blastomeres are stage-specific cell size. The embryo was transferred but did not result in a pregnancy.

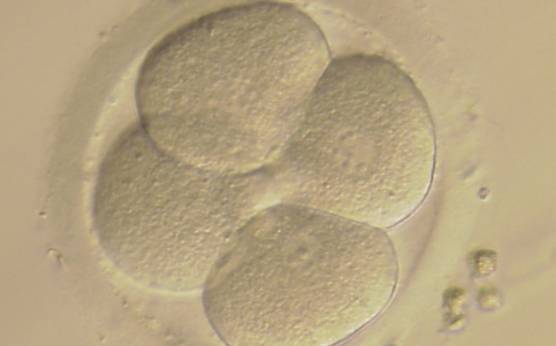
Figure 244
A 4-cell embryo with evenly sized blastomeres and no fragmentation on Day 2. The blastomeres are stage-specific cell size. Notice the clover shape arrangement of the blastomeres. It was transferred and implanted.


Figure 245
An 8-cell embryo with evenly sized blastomeres and no fragmentation on Day 3. The blastomeres are stage-specific cell size. It was transferred and resulted in a pregnancy.
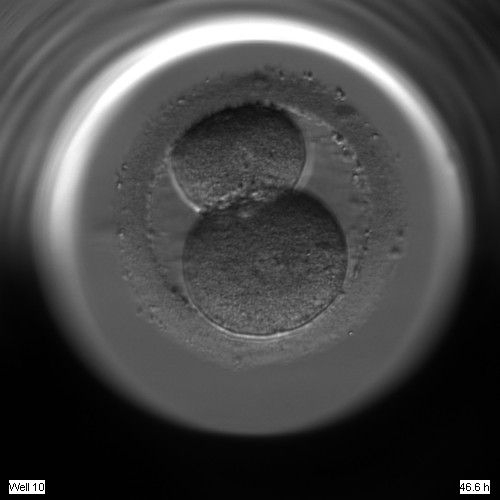

Figure 246
A 2-cell embryo with unevenly sized blastomeres on Day 2. The blastomeres are not stage-specific cell size.


Figure 247
A 2-cell embryo with unevenly sized blastomeres and up to 10% fragmentation on Day 2. The blastomeres are not stage-specific cell size.

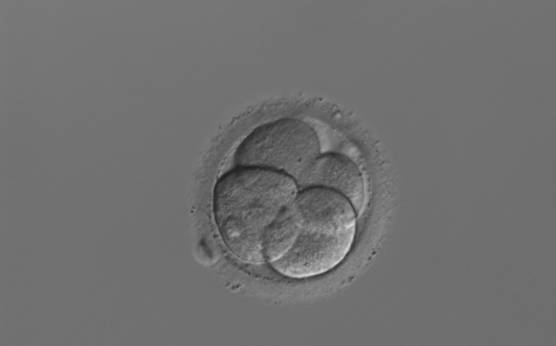
Figure 248
A 4-cell embryo with unevenly sized blastomeres on Day 2, with the cell to the right being 25% smaller than the cell to the left. The blastomeres are therefore not stage-specific cell size. The embryo was transferred and implanted.


Figure 249
A 4-cell embryo with unevenly sized blastomeres on Day 2. One blastomere is indistinct in this view. The blastomeres are not stage-specific cell size.


Figure 250
A 4-cell embryo with unevenly sized and irregular blastomeres with two blastomeres being larger than the other two. The blastomeres are not stage-specific cell size. Note that the ZP of this embryo is elongated.


Figure 251
A 4-cell embryo with unevenly sized blastomeres. The blastomeres are not stage-specific cell size.


Figure 252
An 8-cell embryo with unevenly sized blastomeres. The blastomeres are not stage-specific cell size. The embryo was transferred but did not result in a pregnancy.


Figure 253
A 3-cell embryo with one large and two small blastomeres on Day 2. The blastomeres are stage-specific cell size. The embryo was transferred but failed to implant.


Figure 254
A 5-cell embryo with three large and two small blastomeres. The blastomeres are stage-specific cell size.

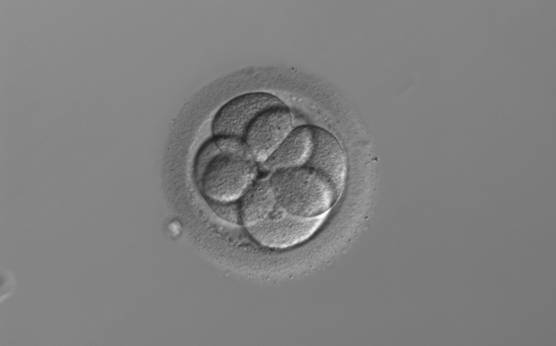
Figure 255
A 6-cell embryo with two large and four small blastomeres. The blastomeres are stage-specific cell size.


Figure 256
A 7-cell embryo with one large and six small blastomeres. The blastomeres are stage-specific cell size.


Figure 257
A 3-cell embryo with three blastomeres of the same size at 26 h after insemination. The blastomeres are not stage-specific cell size.


Figure 258
A 5-cell embryo with two large and three small blastomeres instead of three large and two small blastomeres; therefore, not stage-specific cell size.
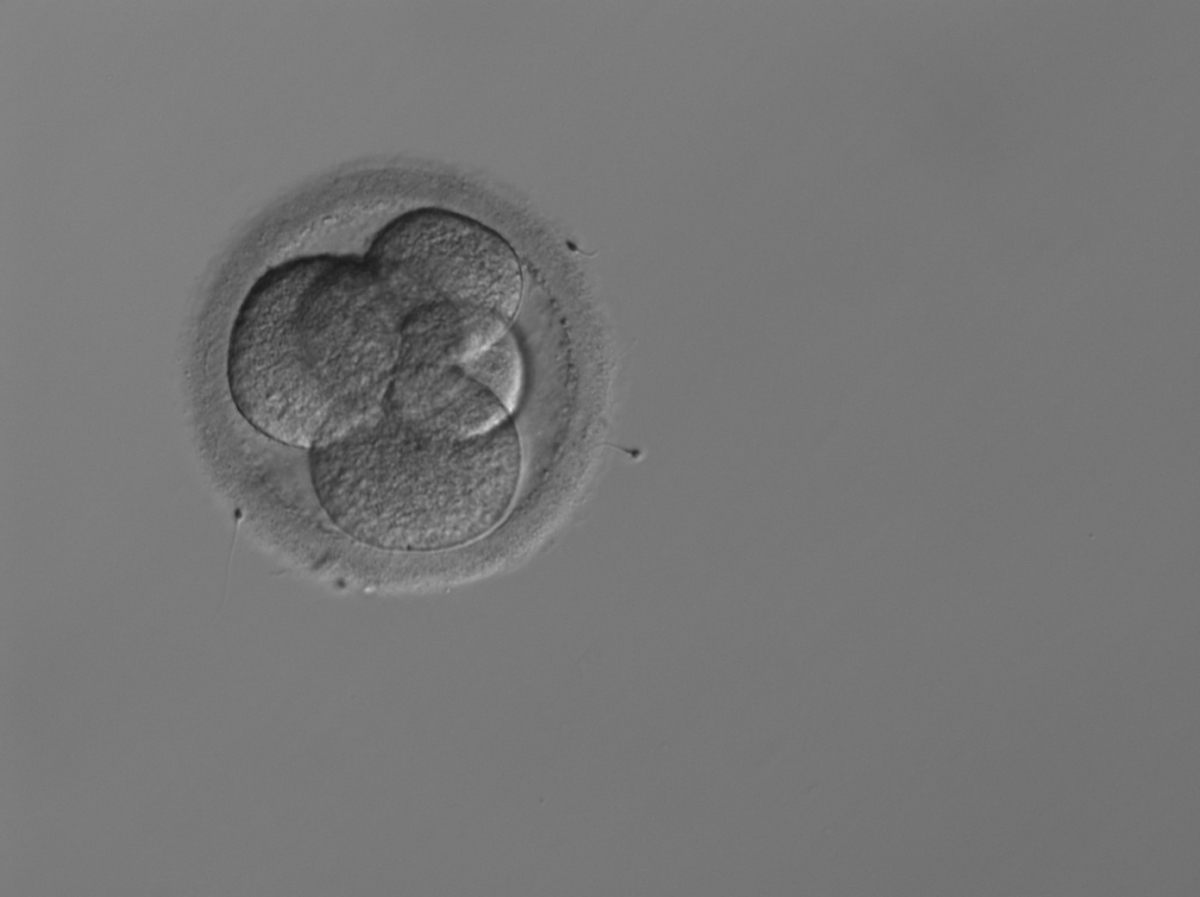
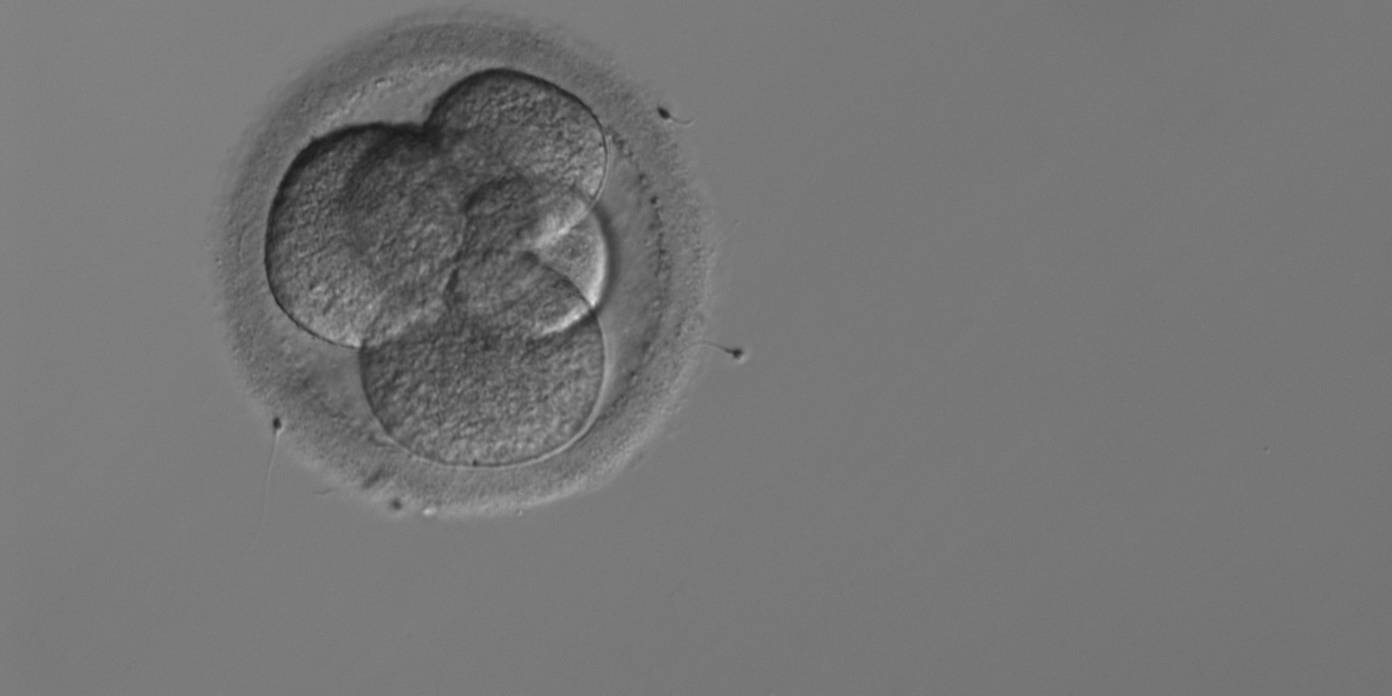
Figure 260
A 5-cell embryo with four large and one small blastomeres instead of three large and two small blastomeres; therefore, not stage-specific cell size.


Figure 259
A 5-cell embryo with two large and three small blastomeres instead of three large and two small blastomeres therefore not stage-specific cell size.


Figure 261
A thawed 6-cell embryo with six blastomeres of the same size rather than two large and four smaller blastomeres; therefore, not stage-specific cell size.
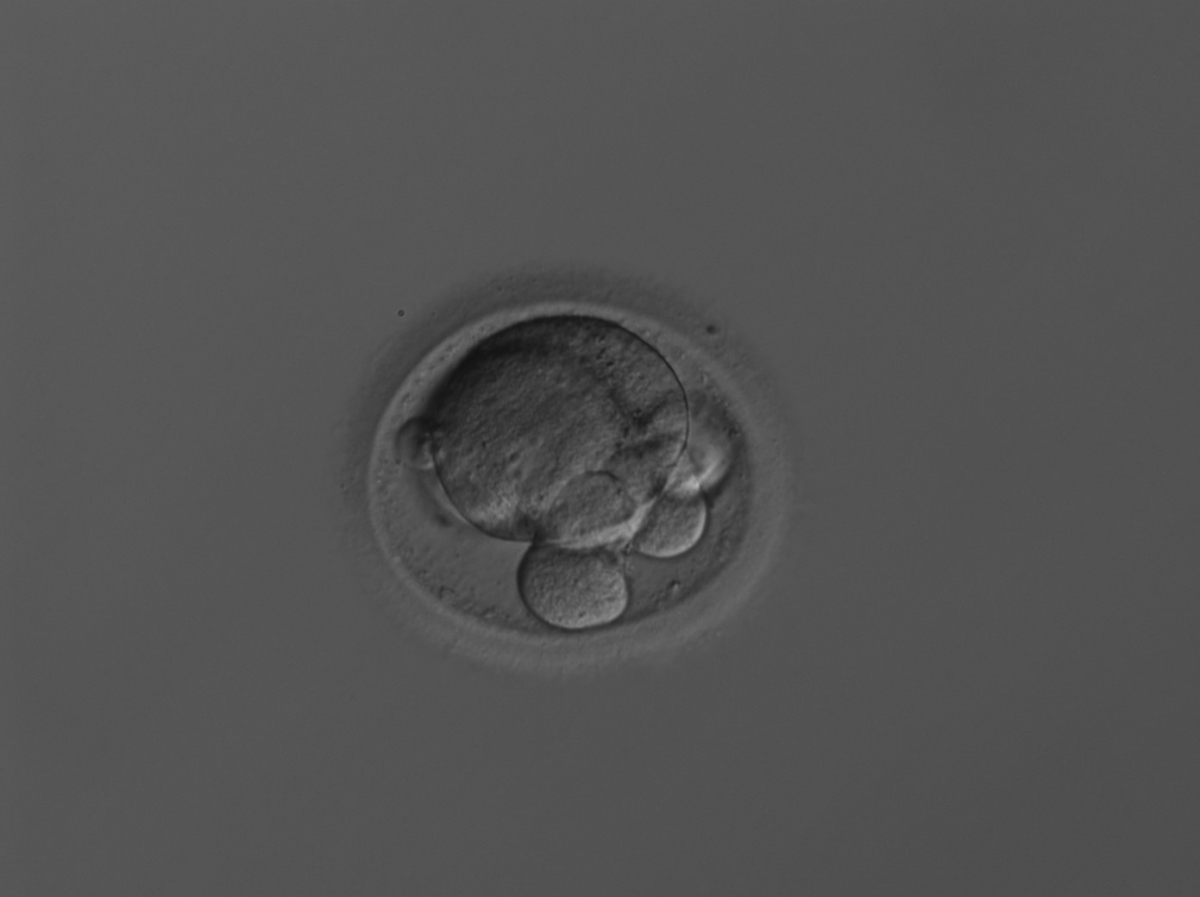
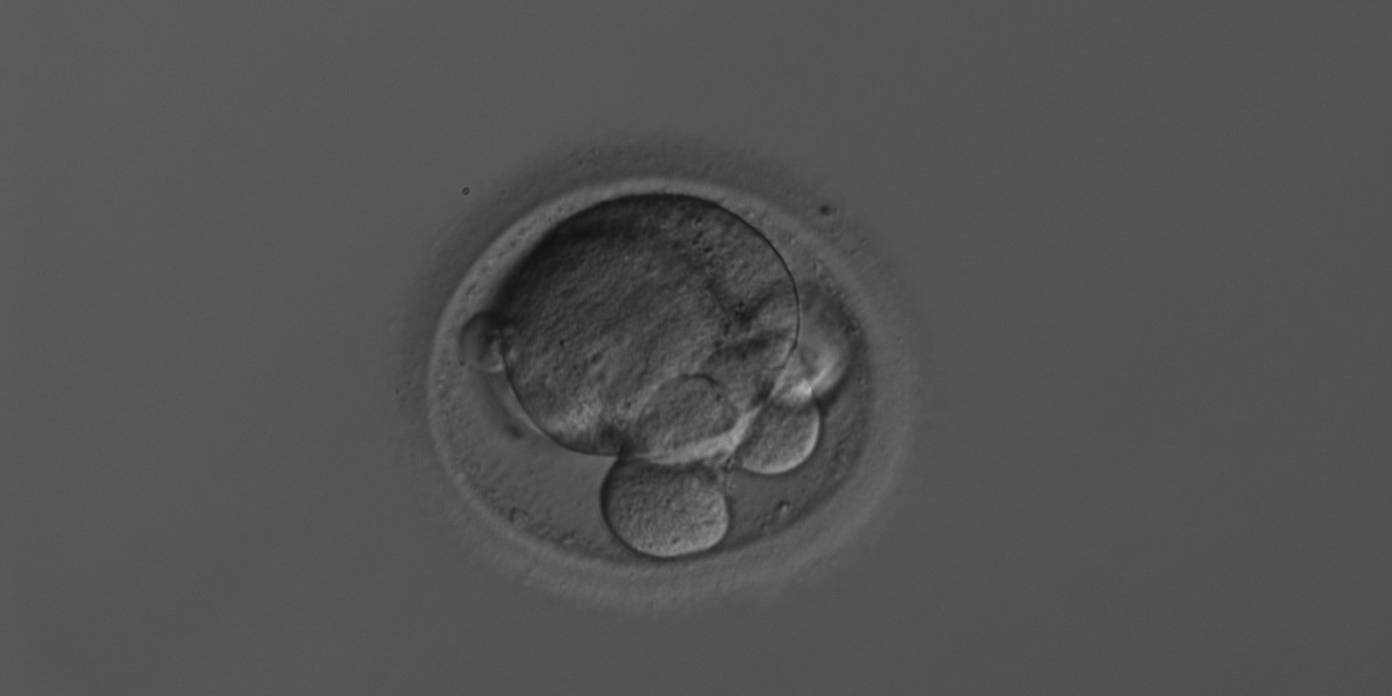
Figure 262
A 6-cell embryo with two very large and four very small blastomeres. The extreme size difference between the large and small blastomeres makes this embryo not stage specific.


Figure 263
A 7-cell embryo with three large and four small blastomeres instead of one large and six small blastomeres; therefore, not stage-specific cell size. One blastomere shows multinucleation.
Article references:
Giorgetti C, Terriou P, Auquier P, Hans E, Spach JL, Salzmann J, Roulier R. Embryo score to predict implantation after in-vitro fertilization: based on 957 single embryo transfers. Hum Reprod 1995;10:2427-2431.
Abstract/FREE Full Text
Hardarson T, Hanson C, Sjögren A, Lundin K. Human embryos with unevenly sized blastomeres have lower pregnancy and implantation rates: indications for aneuploidy and multinucleation. Hum Reprod 2001;16:313-318.
Abstract/FREE Full Text
Holte J, Berglund L, Milton K, Garello C, Gennarelli G, Revelli A, Bergh T. Construction of an evidence-based integrated morphology cleavage embryo score for implantation potential of embryos scored and transferred on day 2 after oocyte retrieval. Hum Reprod 2007;22:548-557.
Abstract/FREE Full Text
Magli MC, Gianaroli L, Ferraretti AP. Chromosomal abnormalities in embryos. Mol Cell Endocrinol 2001;183:29-34.
CrossRef | Medline | Web of Science | Google Scholar
Ziebe S, Petersen K, Lindenberg S, Andersen AG, Gabrielsen A, Andersen AN. Embryo morphology or cleavage stage: how to select the best embryos for transfer after in-vitro fertilization. Hum Reprod 1997;12:1545-1549.
Abstract/FREE Full Text
